













Otoplasty
12 October 2016
Augmentation of the pectorals in men by implants
10 March 2017
By Dr. Lucie DuclosThe author is a plastic surgeon and clinical instructor in the Department of Surgery at the University of Montreal. She also holds a D.E.S.S. in insurance and expertise medicine.
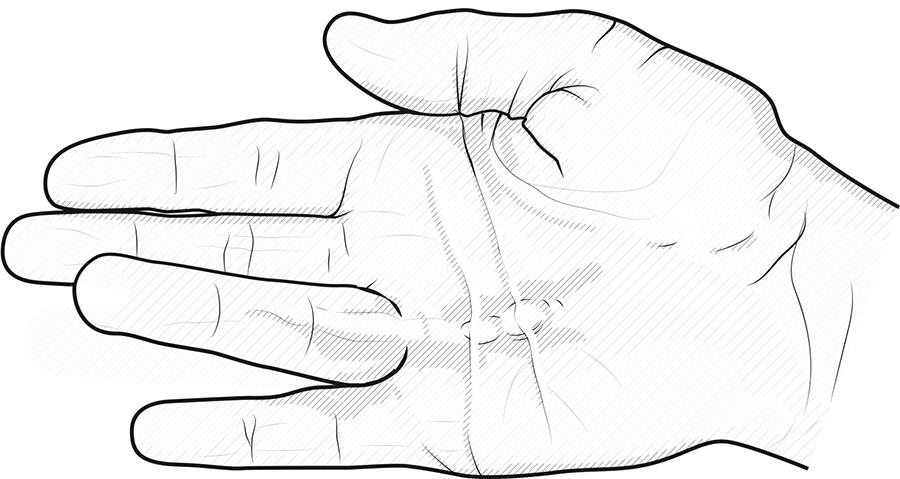
Described in 1831 by Baron Guillaume Dupuytren, this benign “disease” is characterized by the presence of one or more nodules in the palmar aponeurosis. Depending on the progression of the disease, the nodules can form one or more cords and it then becomes increasingly difficult to extend the fingers. Depending on the stage of the disease, sometimes the fingers close completely in the hand.
Until recently, the most common treatment consisted of surgically removing the pathological aponeurosis to allow the fingers to regain better extension. However, this treatment is not without risks, and it has been noted that necrosis could occur, especially in smokers. In addition, a recurrence of the disease is possible, even if the surgical treatment was carried out according to the rules of the art. Several operations on the same site can lead to fibrosis which is accompanied by some difficulty in moving the fingers. In very rare cases, amputation of the affected finger should be considered.

The surgical procedure requires convalescence, which also means a temporary cessation of professional or personal activities. The presence of pain often requires the prescription of narcotics. The surgical wound requires stitches and dressings during the healing process. Finally, physiotherapy or occupational therapy is generally necessary, as is wearing an orthosis in order to maintain the digital extension found after the operation.
There is now a new treatment for Dupuytren’s disease. Less invasive than a conventional operation, this treatment has several advantages and should be systematically offered to patients in order to obtain their free and informed consent.
Exit surgery?
In 2012, Health Canada authorized the use of clostridium histolyticum collagenase, a product already used in the United States and Europe, for the treatment of Dupuytren’s contracture in patients with a palpable cord.
The collagenase is first injected locally into the cord, which relaxes within two days following the injection, whether spontaneously or after manipulation by the doctor. The treated finger thus regains better extension. The number of injections and treatment sessions varies depending on the number of fingers or joints affected. As with surgery, swelling and bruising are possible, and sometimes pain requires a prescription for acetaminophen. Superficial breakage of the skin may occur and require local care. A night orthosis is also recommended for a period of approximately two weeks, but the convalescence is short-lived and the patient can quickly return to their daily activities.
Precision injection
The doctor who administers the injection must have extensive expertise in the anatomy of Dupuytren’s disease. An injection given into other structures of the hand, such as the tendons or ligaments of the hand, can damage them, sometimes even permanently. The same principle applies to all manipulations required in the days following the injection.
Convincing results
A European study compared the complication rate in 1,082 patients treated with collagenase injection and 7,727 patients treated surgically (data from the second group coming from the structured review of 48 studies). According to this study, the incidence of complex regional pain syndrome was 0.1% in the first group, while the median incidence was 4.5% in the second group. Likewise, the incidence of nerve trauma was 0% in the first group compared to a median incidence of 3.8% in the second group. Furthermore, the incidence of infection was 0% in the first group, compared to a median incidence of 4.5% in the second group. According to the authors of this study, most complications occur less often after collagenase injection than after surgery1. Another study evaluated the recurrence rate after five years, which was found to be comparable for injection and surgical intervention2.
In the United States, in 2013, less than 3 years after the introduction of collagenase, the percentage of use of the latter was 20 to 30%, while that of surgical intervention was 60%. A 20% reduction in surgical intervention was noted during this period3.
References:
(1) The Journal of Hand Surgery (European Volume) 2014 – C.A. Peimer, S. Wilbrand, R.A. Gerber, D. Chapman and P.P. Szczypa.
(2) Peimer C, et al. Treatment with collagenase clostridium histolyticum: five-year CORDLESS date. Presented at the International Conference on Dupuytren Disease and Related Diseases. May 22, 2015.
(3) Blazar P, et al. Trends in Dupuytren treatment in the United States. Presented at the International Conference on Dupuytren Disease and Related Diseases. May 22, 2015.



{kind=link}
{kind=link}
{kind=link}